An urgent (but often forgotten) issue in our society is that of the limits to healthcare. Its costs have been on the rise for quite some time now – just a bit, each year, but nevertheless. It will have to stop some time. The problem being: we don’t know how to do so. Moreover: the major pharmaceutical companies are irresponsibly focused on financial gain for shareholders, and that just exacerbates the problem.
Project ‘100 years of antibiotics’
Episode 66. The evolutionary arms race
Episode 67. Technological development, major changes
Episode 68. Limits to healthcare
Episode 69. The future of the pharmaceutical industry in 3 acts, no.1. More of the same
Episode 70. The future of the pharmaceutical industry in 3 acts, no.2. Biology’s promises
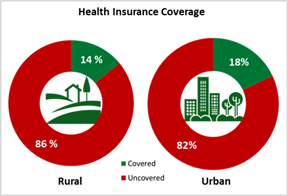
Financial limits
The question into the limits to healthcare has been on our plates for at least fifty years now. We will have to limit the share of healthcare in the national income – but we don’t know how. In most areas, market commodities follow the law of demand and supply. If demand is too large, prices will rise, attracting new entrants to the market, and in the end a new equilibrium will result. Demand determines supply. But in healthcare, it works precisely the other way around (link in Dutch). There, supply determines demand.
Healthcare is in continuous development. In technological respect (our devices become smarter all the time) and also in social respect (people age and require more care, whereas direct relatives supply this to a smaller extent). Demand doesn’t determine anymore the volume of the budget; it’s the other way around: the budget determines the volume of demand. Cures are in growing supply, and demand develops with them. This results in a continuously expanding healthcare, that takes a continuously bigger share of the national income. But the most pressing problem is not in the costs of hospitals. Costs of caring for the elderly and handicapped grow much more. Particularly in our home country the Netherlands, where long-term care is in more ample supply, and better available than in other countries.

Technological development
In our society, people tend not to accept their fate if illness strikes. Many ‘demand’ to become healthy again – a consequence of hyper individualism? This is a strong motor behind much healthcare research. There are lobbies for all kinds of conditions, each with financial resources and technological development centres of their own. Many therapies developed in this vein are quite expensive.
In many areas, for instance in the field of medical equipment, prices still follow the pattern ‘out-of-pocket costs plus a surcharge’. But pharmaceutical companies nowadays determine their prices in a different way. Increasingly, they ask ‘what the market is prepared to carry’. That can be quite a lot, particularly in the case of rare illnesses. Partly, this is because of the insurance system. The rationale of insurances is that the costs of demand can be carried by all insured taken together. We all carry the risk, because the individual risk may be too high; that is the principle of the insurance. But this principle can also be a mechanism through which insurance companies are being cornered. If the lobby (of patients plus pharmaceutical companies) is strong enough, the insurance companies can be forced to pay medicines anyway, even if they are priced far too high.

Market power and how to handle it
Pharmaceutical industry has become very concentrated, with much financial power and with unique products. They have much negotiation power. Research has revealed that from about year 2000 onwards, their strategy has been to gain from this state of affairs. Shareholders made a lot of money from this. This strategy even went so far that major pharma companies made long-term debts (at low interest rates) in order to buy their own shares. They have become moneymaking machines, that have neglected to invest sufficiently in research (link in Dutch) and the production of crucial medicines. This ethically irresponsible behaviour has been described impressively by SOMO, a Dutch foundation that investigates multinational corporations. Here we give a condensed impression of their findings.
Big Pharma increasingly operates like a financial actor
Major pharmaceutical companies (let’s call them Big Pharma) significantly changed their strategy from about year 2000 onwards. They developed more into the field of financial equity; at the expense of their character as production companies of useful medicines. More involved in the business of money making, than of producing medicines.
Research of somo reveals that the financial aspect of Big Pharma grew substantially in the past two decades. They measure this along three dimensions. Firstly, long-term debt of these companies expanded a lot. These loans are used above all for higher payments to shareholders and for the acquisition of innovative companies – not for productive investments in fixed capital or R&D. For the 27 largest pharmaceutical companies, payouts to shareholders (dividends plus share buybacks) grew from 88 per cent of net sales in 2000 to 123 per cent in 2018. In nominal terms, from US$30 billion in 2000 to US$146 billion in 2018. In other words, Big Pharma made long-term debts (at low interest rates) in order to pay shareholders and buy their own shares.
Big Pharma didn’t use the growing debt for productive investments. To the contrary, productive investments declined in this century. And although R&D expenses grew, these were far outperformed by payments to shareholders (link in Dutch). In other words, debt wasn’t primarily used for securing future profits.
All intangible assets on the balance sheet of 27 of the largest pharmaceutical companies increased massively: from 13 per cent of total assets in 2000 to 51 per cent in 2018, standing at a staggering US$857 billion dollars. This shows that producing and selling drugs isn’t the main source of income anymore of Big Pharma. Rather, owning and monopolizing intellectual property.
In sum, says sOMO, Big Pharma creates profits for shareholders on a scale that is socially unaffordable. The payouts to shareholders crowd out essential investments and stifle the conditions for affordable drug supplies. This development has not been unique to the pharmaceutical sector. However, Pharma has an important task in securing the wellbeing of the population. Low interest rates propelled this development; but rising interest rates in the future might endanger the development of new medicines.
The international medicines market has become disturbed. And though people gradually acknowledge this, very little is being done to reset this. If we should set financial limits to healthcare, this is an area that should not be forgotten. Governments will have to set tighter standards for the performance of pharmaceutical companies. Society allows private companies to develop and sell medicines; implicitly however, this implies that this should serve the public good. If that is no longer the case, governments will need to step in. Just to mention an area, many medicines are being developed by major companies on the basis of publicly funded research. This will allow governments to regulate price and availability of medicines developed in this way. Or to set other rules for market entrance and patent protection.
Limits to healthcare
On top of that, we will have to restrict the volume of healthcare as such, sooner or later. Extremely difficult in a democracy. But setting such limits to healthcare happens already, although teeth grinding and in dribs and drabs, there is no other option. We will have to learn this trick. There are conditions that we cannot master, with whatever knowledge. We need to support those struck by them. But we cannot promise them to be healed – even though that is extremely difficult.
But this conflict is about more than the question if we can cover all healthcare costs. A more fundamental conflict lies beneath it – essentially unsolvable and tragic in nature. The clash between individual wishes and limits set by society – here in terms of reach and means of healthcare. This conflict may now be more heated than ever. Around Covid-19, we witnessed that society needs to impose rules in order to protect the community – but that some don’t want to accept such limitations. For some, their individualism is so pervasive that they cannot acknowledge any claims on them, not even when done in the name of the public good.
Fate
Ultimately, our society is in conflict with itself. In the case of healthcare, the conflict revolves around the unwillingness of some to accept limits to care, if this is to the detriment of themselves. Here, individualism conflicts with mutual dependence. Freedom is at odds with regulation. Fundamentally this conflict is characteristic for us as human beings: the (infinite) spirit will have to accept that it is bound to a (finite) body.
Disillusionment
Finally, we end up in disillusionment. During a short interval, say between 1945 and 1970, mankind could live in the illusion that we had developed miracle drugs; medicines that would serve us forever. We then discovered that the conflict with nature will never end. We need to keep on developing. For instance in our medicine kit; the alternative being a healthcare below par. We always need to change, although in a sense this isn’t progress anymore, but a defence of a position taken in the past.
This finally shows the limits to which we can engineer the world. Public culture has grasped this message, but now amplifies it. The world is full of doomsday prophesies, even wars. The climate, pandemics, the formation of elites and wealth gaps, the monetary system, mass migration, plastic pollution, undermining of human autonomy by mass surveillance, shadow realities. This pessimistic world view may be a reaction to unsubstantiated optimism, that ruled the world until the ‘70s. And that also took hold of the medical profession, for a while. Will that propel us into a new economic order like the RethinkX studies suggest to us?
A narrow but passable road
And yet, our task in the conflict with microorganisms is clear enough, in order to return to the main subject of our series. We need to keep developing ourselves and our knowledge. Because we now know that our ‘adversaries’ will keep on developing as well. They do so through natural mutational processes – we do so by continuous research and renovation of our inventory. If we keep this task in mind, we will have come beyond optimism and pessimism. There are no alternatives. We do have to clear up a few obstacles of our own making, like the gigantic costs that companies have to make in order to get a medicine registered. That discourages innovation, and promotes an unhealthy concentration of pharmaceutical companies.
We don’t have to revert to 100 years ago; doctors could then decide if they would test a new medicine on a limited number of patients. But the opposite, testing again and again hundreds of patients in a double blind large-scale investigation, is quite over the top at times. Whatever course we choose, the dilemma will stay with us: do we keep antibiotics in reserve, as much as possible; or do we stimulate the industrial development of new medicines? A national institute that eases out the sharp edges of these choices may seem a good idea, but too often such a institute primarily offers safe jobs for expensive and highly educated researchers, with little social result.
It is a narrow road that we are going to enter. But it is passable, if we should just actively bear in mind the boundary conditions.